Dentofacial deformities are skeletal in nature and affect the occlusion, functions of speech, swallowing, mastication, TMJ function, respiration and digestion. These deformities are often easily and quickly diagnosed by evaluation of the frontal and profile appearance of the patient.
The Pi Dental Care Center in Fort Washington, Pennsylvania is one of the world’s leading resources for cutting edge dental implant treatment and all cosmetic and restorative dentistry.
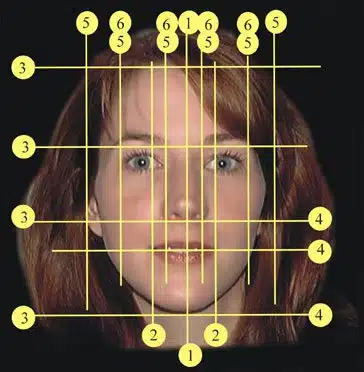
NORMAL FACIAL MEASUREMENTS
1. MIDLINE:
A vertical line drawn through the forehead, nose, upper lip (columella) dental midline and chin that divides the face in half. A variation in right and left side of the face may denote facial mandibular asymmetry.
2. WIDTH OF MOUTH:
Measurement should equal the distance the limbus of the eyes.
3. FACIAL THIRDS:
Face horizontally divided into thirds with lines drawn at the hairline, eyebrow, base of the nose and chin. Approximate normal ratio of the middle third and lower third is 1 to 1.
4. LOWER FACIAL THIRD:
The area between the base of the nose and the bottom of the chin can be subdivided one-third distance from the base of the nose to where the lips meet; and two-thirds distance from where the lips meet the bottom of the chin.
5. “RULE OF FIFTHS”:
The criterion for the perfect face width is five times the width of one eye.
6. ALA BASE:
Width of nose and nostrils equals one “eye width.”
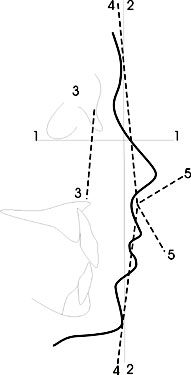
 PROFILE
PROFILE
 PROFILE
PROFILE1. FRANKFORT HOROZONTAL (FH):
The measurement from the top of the external auditory canal to the infraorbital rim which is widely accepted as the horizontal plane of the head. Most profile comparisons are based on this line.
2. ‘O’ MERIDIAN:
A line from soft tissue nasion perpendicular to Frankfort Horizontal. Soft tissue pogonion (most anterior point of the soft tissue chin) should rest 0 to 3mm posterior to ‘O’ meridian.
3. MAXILLARY DEPTH:
An evaluation of the anterior-posterior skeletal positions of the maxilla perpendicular to the Frankfort plane that connects ‘N’ and ‘A’ should equal 0 mm.
4. ANGLE OF FACIAL CONVEXITY:
The 11 degree angle formed by soft tissue glabella (forehead), subnasale (point junction of nose and upper lip) and soft tissue pogonion is an average facial contour.
5. NASOLABIAL ANGLE:
A line tangent to the inferior aspect of the nose passing through subnasale connecting a second line from subnasale tangent to the upper lip. The angle formed between these two lines is influenced by the position of the maxilla. Norm 90 degrees to 110 degrees.
NORMAL RANGE OF LIP MEASUREMENT
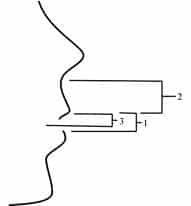 1. INTERLABIAL GAP:
1. INTERLABIAL GAP:
0-3 mm when lips are relaxed.
2. UPPER LIP:
Men 22mm; Women 20mm.
3. UPPER LIP TO INCISAL EDGE:
1 to 4 mm at rest; smile 2/3 to entire clinical crown.
COMMON DENTOFACIAL DEFORMITIES
MAXILLARY DEFORMITIES
Maxillary Hyperplasia Vertical Maxillary Excess or “gummy smile”: overgrowth of the maxillary alveolus in inferior direction; xerostomia; cannot create a lip seal without mentallis strain; often malocclusion.
Maxillary AP Excess: protrusive maxilla; overgrowth in an interior horizontal direction; often class II molar relationship; sometimes combined with mandibular protrusion (bimaxillary protrusion).
Maxillary Hypoplasia Vertical Maxillary Deficiency: edentulous look showing no teeth; short lower face; often combined with deep bite in the mandible and prominent ” chin button.
Maxillary AP Deficiency: inadequate growth in an anterior direction; usually seen in cleft palate and cleft lip; Class III malocclusion; xerostomia, pseudo-prognathism; mandibular excess appearance.
Apertognathia or “Open Bite”: skeletal deformity demonstrating tongue thrust; often speech pattern affected; no lip seal; chronic xerostomia.
Alveolar Cleft: usually occurs with a cleft lip and cleft palate; normally has not been repaired with lip or palate surgery; regurgitation of oral fluids and food into nasal cavity. (Note: Can be repaired at any age, but best done at age 8 to 10.)
MANDIBULAR DEFORMITIES
Mandibular Hyperplasia Mandibular AP Excess: prognathism; Class III malocclusion; maxillary deficiency overlooked in combination with this problem.
Macrogenia: overgrowth of the chin in vertical or anterior direction; often associated with other mandibular deformities; can be isolated.
Mandibular Hypoplasia Mandibular AP Deficiency or “Andy Gump” (very common deformity): deficient anterior growth of mandible; Class II malocclusion.
Microgenia: undergrowth of chin in vertical anterior direction; often associated with other mandibular deformities.
Mandibular Asymmetry: usually excessive growth of one condyle; chin and mandibular midline shift to opposite; malocclusion.
(Note: It is frequently overlooked when evaluating TMJ problems.)
COMBINATION MAXILLARY/ MANDIBULAR DEFORMITIES
Long Face Syndrome: Overall increase of facial height; usually a combination of vertical maxillary excess and mandibular deficiency. (Note: Any combination of the above maxillary and mandibular deformities do exist and are usually corrected at the same time.