Mandibular Bone Height Changes Associated with Screw-Retained Implant-Supported Prostheses with Distal Cantilevers:
A Long Term Follow Up Analysis
Poster Presentation
Thomas J. Balshi, DDS, PhD, FACP*; Glenn J. Wolfinger DMD, FACP*; Matilda Dhima DMD**; Vicki C. Petropoulos DMD, MS**; Stephen F. Balshi MBE*.
* PI Dental Center at the Institute for Facial Esthetics, Fort Washington, PA
** University of Pennsylvania, Philadelphia, PA
Presented at the Academy of Osseointegration Annual Session March 3 – 5, 2011, Walter E. Washington Convention Center in Washington, DC – March 2011.
Introduction: Residual ridge resorption occurs following extractions or loss of teeth. The rate of resorption is variable and considered a multifaceted process including metabolic, anatomic and biomechanical factors. When patients are restored with a removable denture, the residual ridge resorption process does not stop. However, it has been reported in some studies that patients rehabilitated with an implant-supported fixed cantilever prosthesis can not only stop the process, but reverse it.1,2 The longest follow up study available in the literature evaluated these bone changes up to 4 years.
The main purpose of this study was to evaluate the long term changes in bone height of mandibular screw-retained implant-supported prostheses with distal cantilevers and to determine if the reversal of residual ridge resorption in the posterior mandible is only short-term or if it is continued into the long-term management of the patient.
Methods . Panoramic radiographs for each patient were obtained at time of surgery and for two sequential exam visits with varying follow up times. Digital panoramic radiographs were magnified using a computer system with calibrated and known magnification error which was used to convert the pixels into millimeters. The actual implant length and bone height at time of surgery were used as baselines to correct for variation in implant radiographic magnification. Changes in bone height were evaluated between each follow up visit as well as from time of surgery to last follow up. Statistical tests, means, standard deviations, a two way analysis of variation (ANOVA) for the measurements obtained at each exam, and piecewise linear regression model were performed to evaluate the mean changes in bone height between each exam. Characteristics of trends in bone height changes for patient gender were also evaluated.
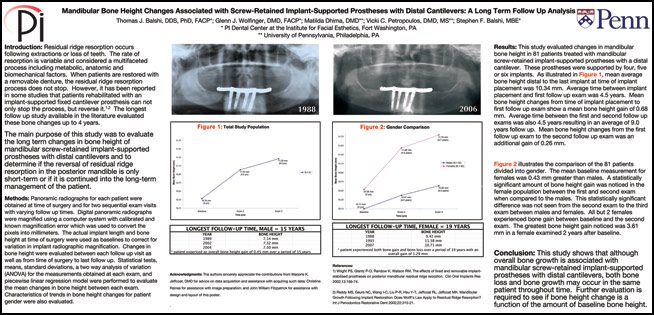
Results: This study evaluated changes in mandibular bone height in 81 patients treated with mandibular screw-retained implant-supported prostheses with a distal cantilever. These prostheses were supported by five or six implants. As illustrated in Figure 1, mean average bone height distal to the last implant at time of implant placement was 10.34 mm. Average time between implant placement and first follow up exam was 4.5 years. Mean bone height changes from time of implant placement to first exam follow up show a mean bone height gain of 0.68 mm. Average time between the first and second follow-up exams was also 4.5 years resulting in an average of 9.0 years follow-up. Mean bone height changes from the first follow-up exam to the second follow-up exam was an additional gain of 0.26 mm.
Figure 2 illustrates the comparison of the 81 patients divided into gender. The mean baseline measurement for females was 0.43 mm greater than males. A statistically significant amount of bone height gain was noticed in the female population between the first and second exam when compared to the males. This statistically significant difference was not seen from the second exam to the third exam between males and females. All but 2 females experienced bone gain between baseline and the second exam. The greatest bone height gain noticed was 3.61 mm in a female examined 2 years after baseline.
Conclusion: This study shows that although overall bone growth is associated with mandibular screw-retained implant-supported prostheses with distal cantilevers, both bone loss and bone growth may occur in the same patient throughout time. Further evaluation is required to see if bone height change is a function of the amount of baseline bone height.
References:
1) Wright PS, Glantz P-O, Randow K, Watson RM. The effects of fixed and removable implant-stabilised prostheses on posterior mandibular residual ridge reorption. Clin Oral Implants Res 2002;13:169-74.
2) Reddy MS, Geurs NC, Wang I-C, Liu P-R, Hsu Y-T, Jeffcoat RL, Jeffcoat MK. Mandibular Growth Following Implant Restoration: Does Wolff’s Law Apply to Residual Ridge Resorption? Int J Periodontics Restorative Dent 2002;22:315-21.